- SELF STUDY MODULES
- 1. Intro to TBI
- 2. Communication
- 3. Skills for independence
- 4. Cognitive changes
- 5. Behaviour changes
- 6. Sexuality
- 7. Case management (BIR)
- 8. No longer available
- 9. Mobility & motor control
- 10. Mental health & TBI:
an introduction - 11. Mental health problems
and TBI: diagnosis
& management - 12. Working with Families
after Traumatic Injury:
An Introduction - 13. Goal setting
- 13.0 Aims
- 13.0A Take the PRE-Test
- PART A:
SETTING GOALS
IN REHABILITATION
- 13.A1 Goal setting in rehabilitation
- 13.A2 Goals, steps and action plans
- 13.A3 Goal setting in Person centred care
- 13.A4 Person centred/directed planning & goals
- 13.A5 Participation
focus & goals - 13.A6 Effective Goals
- 13.A7 SMARTAAR Goals: Characteristics
- 13.A8 Tips for Funders and Services
- 13.A9 Take home messages
- PART B: TEAMS &
GOALS - PART C: WORKSHEETS
- PART D:
POST-TEST
AND RESOUCES
13.A5 Participation focus and goals
- (i) Participation
focus and goals - (ii) Types
of goals (ICF) - (iii) Examples
of Impairment /
Activity/ Participation of goals - (iv) Participation and
impairment goals
Participation focus and goals
There are many factors that influence the nature and size of goals that are written to support rehabilitation.
The primary approach used in this Module to describe different levels of goals is the World Health Organisation (WHO) International Classification of Functioning, Disability and Health (ICF).47
This provides a useful framework for describing and understanding the primary focus of rehabilitation goals. Within this rehabilitation goals can be set at three
levels that describe the desired change in the person’s:
1. level of impairment
2. level of activity
3. level of participation.
Wade in 2009 notes that goals are most helpful for clients when they address priorities that are important to them. Clients may identify participation, activity or impairment level intentions or priorities, but extending the conversation will identify how this will impact on their life.
The achievement of valued and meaningful outcomes is dependent on the integration of our therapeutic interventions focussed on the participation level described by the ICF.
What are example of impairment goals?
What are examples of activity goals?
What are examples of participation goals?
The International Classification of Functioning, Disability and Health (ICF)
The International Classification of Functioning, Disability and Health (ICF) (2001) and classifies the consequences of health conditions on functioning.
The components of the ICF model include:
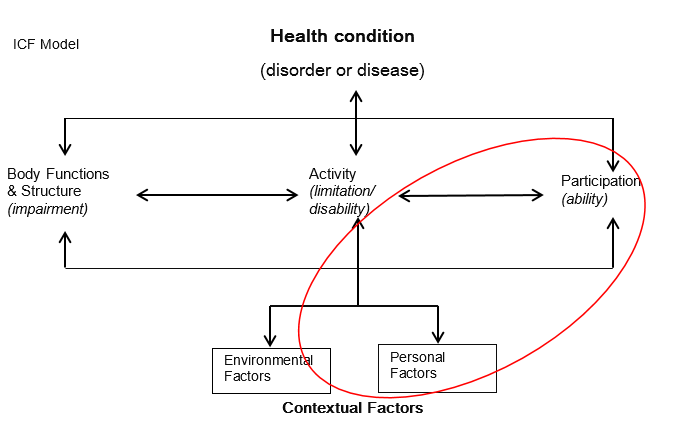
Body function and structures
Body function and structures: refers to physiological functions of body systems (including psychological functions) and anatomical parts of the body (including organs, limbs).
Impairments occur when people experience problems at the level of body function and structures.
Activity
Activity: describes the execution of a task or action by an individual. Problems with activities are described as activity limitation.
Participation
Participation: describes involvement in a life situation. At the level of participation, the activities and behaviours people engage in are performed in relation to their roles and the context in which they live. Problems with participation are described as participation restrictions. People can experience participation restrictions due to the impact of impairments, activity limitations or contextual factors e.g. prejudicial attitudes, lack of services, inaccessible environments.
Disability
Disability is an overarching term that describes a problem at any of the three levels.
Contextual factors
Contextual factors: describe aspects of the environment in which a person lives that can be thought of as facilitators and barriers to functioning and participation. Contextual factors include environmental factors (e.g. social attitudes, architectural characteristics, legal and social structures, climate, terrain) and internal personal factors (including gender, age, coping styles, social background, education, profession, past and current experience, overall behaviour pattern, character).
The ICF is a biopsychosocial model that acknowledges that the experience of health is dynamic, where change in one component can impact others. In rehabilitation, intervention can target each aspect of the model, including the context / environment in which people live.
Examples of Levels of goals
The ICF provides a useful framework for articulating the desired and different levels of
rehabilitation goals. Using ICF terminology, rehabilitation goals can be set at three
levels that describe the desired change in the person’s:
1. level of impairment
2. level of activity
3. level of participation.
This concept is most easily explained through examples.
Impairment |
Activity |
Participation |
Kate will be able to comprehend a 5-step written instruction |
Kate will be able to follow a recipe to make a cake |
Kate will contribute to her son’s school fete by supplying 4 cakes |
Steven’s hip extensor strength will increase from 3/5 - 4/5 |
Steven will be able to independently transfer from wheelchair to car |
Steven will be able to join his mates at their weekly outing to the pub |
Joanne’s anxiety will decrease by 3 points on the DASS |
Joanne will be able to be in the company of unfamiliar people for >45 minutes without experiencing an anxiety attack |
Joanne will attend her daughter’s ballet recital |
David’s deep neck flexor strength will improve from grade 2 to grade 4 |
David will be able to work at a computer for 4 hours without experiencing pain greater than 3/10 |
David will return to work 4 hours/day, 3 days/week |
Using the examples in the Table above, Steven’s physiotherapist will be interested to measure improvement in his hip extensor strength to check that Steven is responding to therapy as planned and to guide when an attempt at independent transfer might be appropriate.
Similarly, Joanne’s psychologist might measure anxiety using the Depression, Anxiety and Stress Scales (DASS) scores over time to determine the effectiveness of the psychology sessions and guide when it might be appropriate for Joanne to expose herself to different challenges.
However, the more meaningful outcome for Joanne will be whether she is able to attend and enjoy her daughter’s ballet recital – her main priority.
Participation goals
Participation level goals are considered best practice in rehabilitation.
The ICF concept of participation is consistent with the aim of rehabilitation to reduce disability and ‘make life worth living’. In Australia, ‘the rehabilitation process is different for everyone and rehabilitation programs should be individualised, catering to each person's unique needs’.
Participation anchors activity performance in the context in which the person lives.
Participation level goals are more likely to motivate clients as they demonstrate how rehabilitation can help them achieve meaningful outcomes. For example, telling a client physiotherapy for 8 weeks will enable them to commence a trial to return to driving is likely to be much more motivating than the potential to improve their neck rotation by 30o.
Impairment goals
While participation-level goals are advocated as best practice, and are most likely to reflect the longer term priorities of clients, at times impairment goals can also be appropriate.
This is particularly the case in the early stages of recovery and when level of disability remains severe.
The focus of a large proportion of therapy in these situations often addresses impairments. The level of engagement of clients in the rehab process is often lower when the client’s level of disability is more severe, so setting participation-level goals is more difficult, are less likely to be achievable in short term, and rely on family members’ views of what’s important to the client. However, even during the early stages, it is important to engage clients as much as possible in identifying their priorities for meaningful activity- and participation-level goals. This does not mean that impairment-level goals need not be identified and addressed. Ideally, they will support the client to achieve activity- and participation-level goals, or provide mechanisms to measure progress.
For example, an elderly client may not have regained the last 20o of shoulder range of motion, but if he is satisfied with his ability to perform all desired activities, this impairment becomes irrelevant in guiding treatment. Conversely, a client who wishes to return to playing tennis may have only lost 10o of shoulder range of motion, but the restoration of full range may be vital for the achievement of her goal of return to tennis.
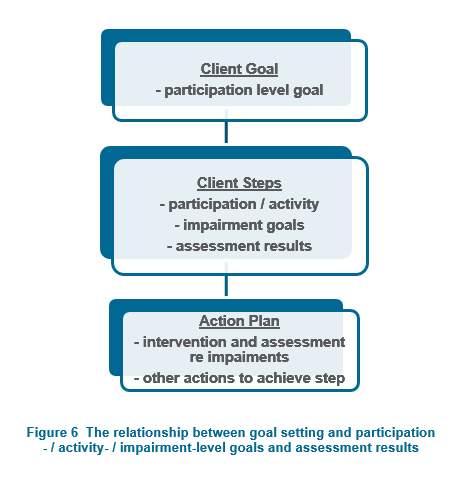
Impairment-level goals are generally more useful for directing and assessing discipline-specific interventions. This may be accompanied by impairment level objective assessments to provide detailed clinical information on current status and treatment needs. Impairment goals may be reported as steps, or in the action plan where therapy and assessments to address impairments are described. Figure 6 illustrates this relationship.
Contextual factors
While contextual factors can often be addressed as part of rehabilitation, they should usually be described in action plans that support achievement of client change at the level of activity or participation as appropriate e.g. provision of equipment and therapy is a contextual factor in the ICF and an action that supports the client to achieve their goal.