- SELF STUDY MODULES
- 1. Intro to TBI
- 2. Communication
- 3. Skills for independence
- 4. Cognitive changes
- 5. Behaviour changes
- 6. Sexuality
- 7. Case management (BIR)
- 8. No longer available
- 9. Mobility & motor control
- 10. Mental health & TBI:
an introduction - 11. Mental health problems
and TBI: diagnosis
& management - 12. Working with Families
after Traumatic Injury:
An Introduction - 13. Goal setting
- 13.0 Aims
- 13.0A Take the PRE-Test
- PART A:
SETTING GOALS
IN REHABILITATION
- 13.A1 Goal setting in rehabilitation
- 13.A2 Goals, steps and action plans
- 13.A3 Goal setting in Person centred care
- 13.A4 Person centred/directed planning & goals
- 13.A5 Participation
focus & goals - 13.A6 Effective Goals
- 13.A7 SMARTAAR Goals: Characteristics
- 13.A8 Tips for Funders and Services
- 13.A9 Take home messages
- PART B: TEAMS &
GOALS - PART C: WORKSHEETS
- PART D:
POST-TEST
AND RESOUCES
13.A4 Person centred planning & goals
- (i)
Person centred /
directed planning - (ii)
What it
looks like - (iii)
Types of
goals - (iv)
Client
Generated - (v)
Client
Focussed - (vi)
Clinician
Goals
Person centred / person directed planning
There is a trend in health care around the world to shift the locus of decision making towards the client.
This trend can be seen in the following diagram.
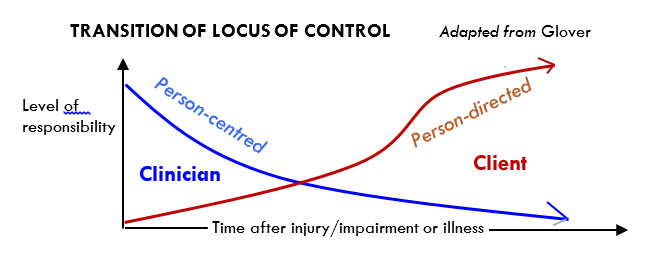
Best practice starts with person-centred goals and moves to person directed goals.
As with the words goals, steps and action plans there is different language is use.
Here we look at Person centred / person directed planningand within that context look in more detail at what are often referred to as:
- Clinician goals
- Client focussed goals
- Client generated goals
What does person-centred / directed planning look like?
- A partnership with the person, their ‘close others’ and the team
- Tailored to the needs and aspirations of each individual (not standardised to their condition or conditional on what your service usually provides)
- The person brings to the partnership who they are, their values, past experience and knowledge
Communication in a person-centred model:
- Health workers able to describe the processes in terms the person and family will understand
- Communicate effectively using words the person will understand; construct valid and meaningful goals for the person (e.g. techniques such as Motivational Interviewing).
- Doesn’t mean having to use the word “goal”. What other terms might identify the outcome of value to the person? (Feeney: valued outcome; others describe ‘priorities, aims, desires.)
- What would your life look like if you were happy?
- “What would you like to be doing when you are happier?”
- “What would you like to be able to do?”
- “How will you know when to stop coming here/seeing u
Sometime asking the client simple questions can often be most useful,
What are the most important things in your life?
What were you planning to do /what were you doing before you had your accident?
What things do you want to be able to do that you can’t do now?
Client says “I want to be happy” –
Develop questions and interview styles that work for you.
E.g. “Tell me about your life in the month before you came to hospital?”, mapping priorities.
Look up Ylvisaker/ Feeney scripts: “So you want to be able to..(e.g. get a job), but let’s think about what you need to be able to do to make this happen (e.g. catch the bus, manage 8 hours of activity, buy lunch, deal with difficult customers, lift heavy loads….”) and use these to develop realistic smaller goals that are still relevant to the client’s priorities).
Ask the person or the family: What’s the ONE thing that would make a difference?
Plan for transition (and shift of control from family to client) as the person recovers.
Person centred also considers equitable access to appropriate services.
Example of “equality” may be that everyone is given insulin; “equity” means that people who do not produce enough insulin to regulate sugar metabolism, are given the dose that they need.

Types of goals and client engagement
Client engagement in the goal setting process falls on a continuum.
At the highest level of engagement, the client will generate their own goals, or some of their own goals.
Which of the following are true?
However, sometimes rehabilitation needs to support the client achieve other goals, even when they have not been explicitly identified by the client themselves. For example, when clients have identified a long term goal but have been unable to identify shorter term goals for funding requests that will enable them to achieve their longer term goal. Similarly, a client may not be able to identify all of the steps that will be needed to achieve their goal.
At the other end of the continuum clinicians identify goals but these tend not to describe how the client will benefit.
The impact of client factors on client engagement are dynamic, and an individual client may be able to identify some but not all goals, so their level of engagement in identifying goals will vary from goal to goal.
The three levels on this continuum of client engagement are:
- Client-generated goals
- Client-focused goals
- Clinician goals
Both client-generated and client-focused goals describe an expected outcome i.e. how the client will change / benefit at end of the proposed rehabilitation, but client-generated goals describe the client’s own priorities.
Client-generated and client-focused goals both involve a level of collaboration with the client and support client-centred rehabilitation.
Client generated goals
A client generated goal is one that the client identifies - it reflects their priorities.
The goal may or may not be as stated verbatim by the client. It may have been formulated or re-worded by a health professional to maximise the usefulness of the goal statement but it directly relates to the anticipated level of change desired by the client.
Ideally, a client generated goal can be reported verbatim in the client's own words but, in most rehabilitation situations, the health professional will need to assist in the formulation of the goal statement.
The health professional makes improvements to the goal in order to generate a statement that is useful for directing intervention, communicating the rehabilitation plan with all stakeholders and measuring progress towards the goal.
When the client’s own words need to be changed to fulfil the needs for the goal, the client should be involved as much as possible in translating their priorities into a SMART rehabilitation goal. It should still be something the client understands and agrees to.
Client focussed goals
A client focused goal is one that one that still relates to how the client will benefit from the therapy, but may not be an explicit priority identified by that client.
These can often be steps that help the client achieve their client generated goal.
Client focused goals can be set by the clinician but still describe how the client will benefit from therapy. They can be useful to identify additional changes in activity or function that are required for the client to achieve their own goal e.g. encouraging the client to shower daily as a strategy to support their ultimate goal of ‘getting a girlfriend’. In this example, the client may not be able to identify what a realistic goal is for their particular situation, or may fail to understand the link between shorter term goals and their ultimate goal of ‘a girlfriend’.
Many factors, including insight, adjustment to disability and time since injury, affect a client’s ability to set a realistic goal. When clients identify goals that are unrealistic, or cannot be achieved in the foreseeable future, client focused goals may need to be set to support rehabilitation planning. As clients gain insight and understanding, the client may become able to identify the importance of these goals.
Clinician goals
Clinician goals are on the other end of the continuum and usually describe what needs to be done and by when – often what the client will be doing in therapy e.g.
- ‘Jack will complete his home exercise program’,
- ‘Jill will complete 6 sessions of physiotherapy’,
- ‘Jack will achieve 5 point change on assessment scale’.
Clinician goals often describe what the clinician wants the client to do, but are distinguished from client focused and client generated goals which focus on how the client will benefit from therapy.
Clinician focused goals can be appropriately reworded in the action plan, as these typically describe actions to support the client achieve their own goal.
They can also provide opportunities for monitoring progress against the client’s goals e.g. if the client achieves the clinician generated goal of being able to ‘sit for 30 minutes without pain’, they are likely to be closer towards being able to achieve their own goal of managing their office work. The client’s progress towards goal achievement can be monitored by using a standardised assessment at regular intervals.
Clinician goals are less likely to reflect the client’s own priorities and may / may not describe the anticipated change in a client.