- SELF STUDY MODULES
- 1. Intro to TBI
- 2. Communication
- 3. Skills for independence
- 4. Cognitive changes
- 5. Behaviour changes
- 6. Sexuality
- 7. Case management (BIR)
- 8. No longer available
- 9. Mobility & motor control
- 10. Mental health & TBI:
an introduction - 11. Mental health problems
and TBI: diagnosis
& management - 12. Working with Families
after Traumatic Injury:
An Introduction - 13. Goal setting
- 9.0 Aims
- 9.0A Take the PRE-Test
- 9.1 Brain injury and motor symptoms
- 9.2 Common physical presentations
- 9.3 Role of physiotherapy
- 9.4 Physiotherapy interventions
- 9.4a Motor retraining
- 9.4b Prevention of secondary complications
- 9.4c Fitness training
- 9.4d Regular physical activity
- 9.5 How can carers help make physiotherapy happen
- 9.6 Minimising risks
- 9.7 Take home messages
- 9.8 Resources
- 9.9 Take the POST-test
9.1 Brain injury and motor symptoms
i) Introduction
How does the location of the brain injury affect motor function?
Injury to the nervous system produces many motor symptoms, ranging from paralysis of one or a few muscles to generalised difficulties in planning and co-ordinating complex movements.
To understand the connection between the brain injury and the motor impairments that you see it is useful to understand a little about the anatomy of the skull and the brain.
If you have completed Module 1 you will have covered the material on the ii) Skull & iii) the Brain
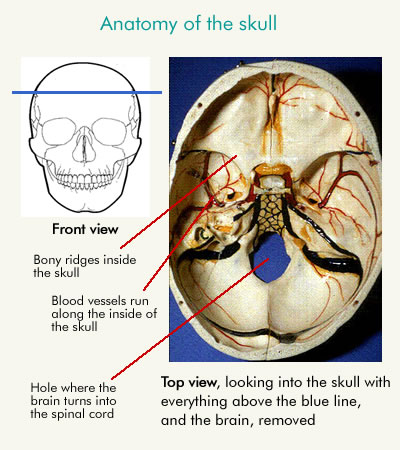
ii) Anatomy of the skull
The skull is a hard, bony box protecting the brain. It fits neatly around the brain, with the brain sitting inside, floating in cerebrospinal fluid.
There are a number of bony ridges that are on the inside of the skull that fit into gaps in the brain. These ridges can cause damage to brain tissue in the event of a TBI. This damage can commonly include lacerations or contusions around the frontal/ temporal lobes and contra-coup damage in the region of the occipital lobe.
Blood vessels line the inside of the skull, and there is a hole (the foramen magnum) at the base of the skull where the brain becomes the spinal cord.
iii) Anatomy of the brain
The brain is made up of two different types of tissue:
- Grey matter: which is groups of nerve cells that form layers of soft grey tissue
- White matter: which is long fibres that connect different groups of cells and have the consistency of al dente spaghetti or jelly
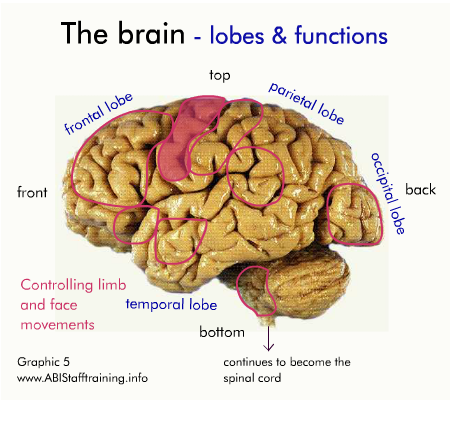
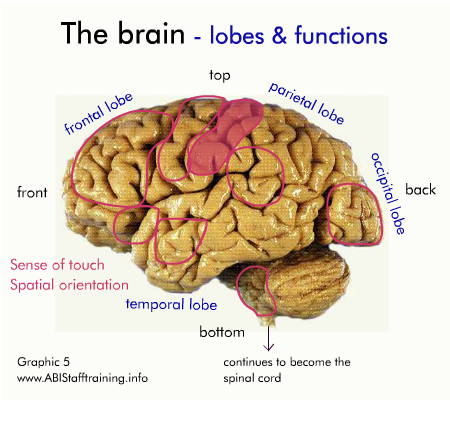
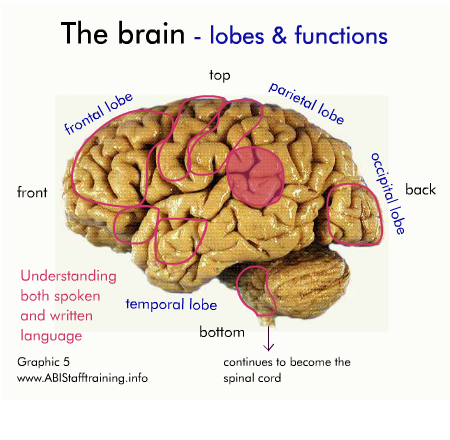
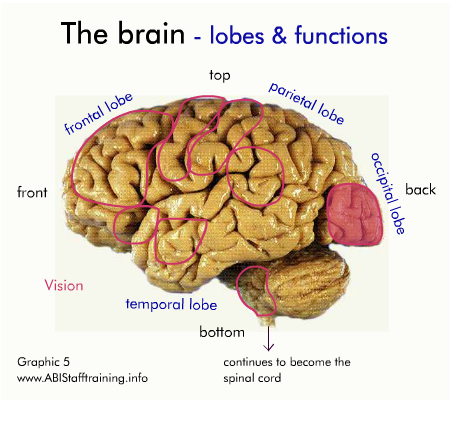
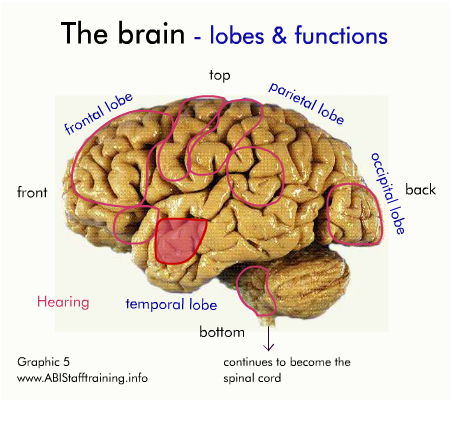
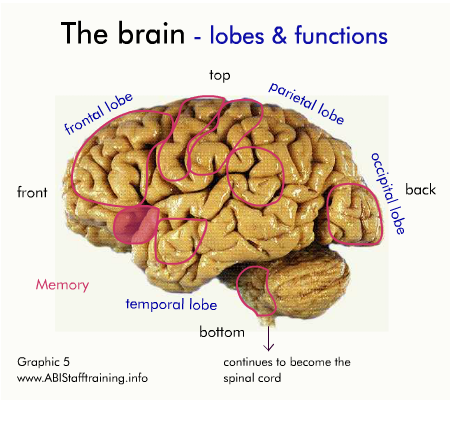
The brain has a left and right hemisphere. Each hemisphere controls the opposite side of body. The left side also usually controls understanding and production of speech. Each hemisphere is divided into 4 lobes - frontal, temporal, parietal, occipital. Different lobes, and different areas within each lobe, control different functions.
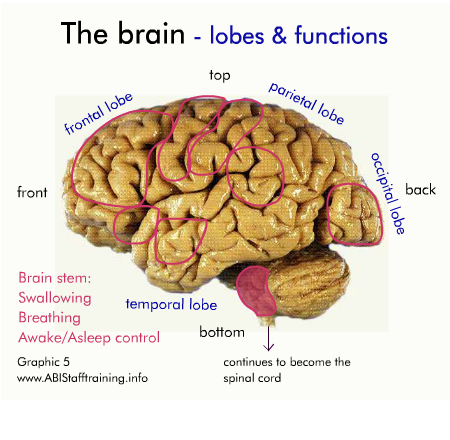
At the base of the brain, just above where it turns into the spinal cord, is an area called the brain stem. The brain stem controls our vital functions such as breathing. If the brain stem is damaged it can be extremely life threatening.
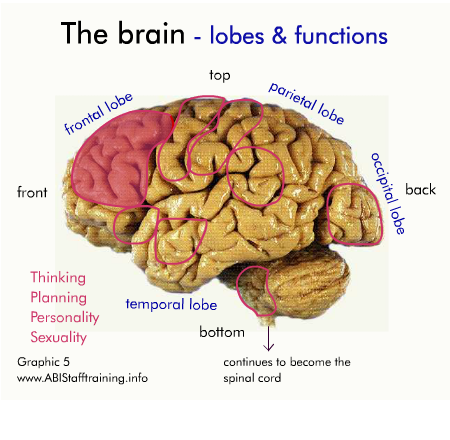
Many of the things we do depend on several functions, which means several of these areas must work together. For example, in order to follow the direction "put your socks on" you need to use the following areas:
- the area for understanding language, in order to understand the direction
- the area for spatial orientation, to be able to find your sock
- the area for controlling limb movements, in order to put your sock on
- and the area for planning in order to be able to plan these steps and execute them in the correct order
To allow the different areas of the brain to work together, the brain has networks of nerve fibres that connect the areas together. There are also nerve fibres that connect the brain to the rest of the body, allowing it to control the activities of the person. If either the area that controls a function in the brain, or the nerve fibres that connects that area to the rest of the brain or to the body are damaged, a person will have difficulty performing that function.
For example, some people believe that if their arm or leg does not work, then there is a problem with the arm or leg itself. However, after a brain injury, the arm or leg may not work as a direct result of damage to the area of the brain controlling this movement or any of the nerve fibres that connect the brain to the limb.
iv) Effects of injury
Injury to the nervous system produces numerous motor impairments, ranging from focal paralysis of one or a few muscles to generalised difficulties in planning and co-ordinating complex movements.
The main line of the motor system consists of pathways between the spinal cord, brain stem and motor areas of the cerebral cortex. This is know as the Upper Motor Neuron System.
Lesions to the Upper Motor Neuron System may result in an enhancement of some features (positive features) or a reduction in others (negative features).
Positive features can include:
Hyperreflexia (claspknife phenomenon, exaggerated tendon jerks, clonus) Hypertonus (abnormal resistance to passive movement)
Negative features can include:
Loss of strength Loss of dexterity Fatiguability
Spinal systems
Lesions in the spinal system lead to: - loss of voluntary control (focal paralysis and weakness) - loss of sensation - disorders of tone (hypertonicity or hypotonicity) - complex reflex patterns or poor postural control
Brain Stem System
Brain stem lesions lead to: - dyscontrol of automatic behaviours, such as posture, locomotion and breathing.
Motor Areas of the Cerebral Cortex
Lesions to the motor cortex or its descending projections cause: - weakness - hyperreflexia - spasticity The motor cortex plays an important role in organising, shaping and refining movement
Cerebellum
Lesions in the cerebellum leads to: - poor planning of movement - poor regulation and timing of movement - reduced smoothness and co-ordination of movement
Basal Ganglia
Lesions of the basal ganglia cause: - slowing of movement - poor co-ordination - poor implementation of motor plans
Association Areas of the Cortex
Association areas are involved in higher perceptual and cognitive functions as well as complex behaviour and language.
Peripheral System
Lesions in the peripheral system of the nervous system lead to: - focal weakness - loss of sensation.
![]()